A breeze in Borneo lifts your spirits, brings sanity to the sultry heat and lets you look at things differently. It can waft right through your day.
Thursday, January 11, 2007
Peregrinations with Camels
Camels bearing their precious cargo, weaving in and out of traffic on the dusty highways, their colorful tassels swinging, capture for me the contradictions of our Pakistani health project. The exotic melds with the mundane. The amazingly simple rests cheek-by-jowl with the incredibly complex. And perception is in a constant dance with reality.
Our project has two main goals. The first, which has a well-worked out and detailed work plan, looked initially to be the simplest. It is to strengthen the management of STD in 30 health units North Western Frontier Province of Pakistan. Because the early results from our initial baseline survey have revealed that blood products are not screened, sterilization is inadequate, placentas are handled in ways that put health workers at risk and not all health units are staffed, this seemingly simple goal may prove to be much more complicated than first envisioned. The second goal is to build an ongoing, productive and flourishing partnership between the Canadian partner, the Society of Rural Physicians of Canada and the Pakistani partner, Frontier Primary Health Care. The second goal is somewhat more difficult to pin down and hard to measure, but may in the end prove to be the simpler. Reality and perception are in a constant, interchangeable dance around elusive truth. Frontier Primary Health Care (FPHC) is a Pakistani Non-Government Organization (NGO) providing health care to 180,000 people in 3 different districts. They have 120 staff, 5 health centers, 3 literacy centers for young girls, a basic obstetrical unit and a Community Development Project. Frontier started in the health business with 3 Afghan refugee camps in 1981. Their success was such that they were invited to extend their services to surrounding Pakistani communities. Success in such situations is measured in part by how well health interventions manage to lower things such as maternal mortality and to improve health and treat illness in children under the age of five. We are lucky to have such an experienced and able partner. They could do the project without Canadian input. They are used to working in a system where rigorous purdah is practiced. They utilize community and religious leaders effectively to improve health in their communities. With a committed army of both male and female volunteers, they are able to reach almost everyone in the community regularly. One of the value-added pieces that Canadian physicians can provide, they tell us, is assistance in writing funding proposals and preparing reports that would make their work better known.
For their work in refugee camps, FPHC has been funded mainly by United Nations High Commission for Refugees (UNHCR). Among the Pakistani population surrounding the camps, the medical services provided are made sustainable through modest user fees, or what is called in development parlance, “cost recovery”. Many of the Afghan refugees have been in Pakistan for more than 25 years. The younger generation of refugees has been born in Pakistan. And UNHCR is experiencing "donor fatigue", so FPHC needs to find other donors and to ensure that the services provided are sustainable and can be afforded by the population. This is both simple and complex. It is a specific, measurable objective and therefore straight forward. Difficult, in that navigating the vicissitudes of international funders and locating appropriate donors occupies the time and energy of whole legions of people in aid agencies. If we manage to accomplish this one thing, however, we will have made our partnership worthwhile. So we already working on our next project and are on the outlook for potential donors.
Pakistan is under tight security currently so outsiders are not allowed into the refugee camps. Because Frontier PHC operates health units which are often located in the middle of the camps, staff are allowed to move to and from the health unit but not to stop in the camp enroute. During my recent visit, I was attempting to take pictures of children working in the sugar cane field and asked if we could stop on the road.
“No,” I was told sternly by staff, “We cannot stop in the camps.”
Moments later right in front of us, a donkey who was drastically overloaded, collapsed on the road, feet splayed out in front of him and would not budge. In the kafuffle that ensured, a group of laughing Afghani boys hauled on the donkey, trying to tug him upright. They placed the donkey’s legs under him, but as soon as they removed their hands, he collapsed again in a heap. Motorbikes and lorries loaded with sugar cane backed up behind us on the narrow dirt lane, beeping their horns. The donkey however was going nowhere.
Our staff laugh and tell me me that now I can take an even better picture. This is one of the contradictions of our project. Prohibitions exist and are strictly enforced but then along comes a commonplace, uncontrollable event and the situation is dramatically changed in the blink of an eye. One of the things Maggie, a physician colleague, and I were asked to do during our visit was a review of obstetrical cases. A review of cases is called a medical audit. When something goes badly wrong in medical care, the result is often that someone dies or gets a complication. So audits, while necessary, can be difficult and discouraging undertakings for physicians. The staff of the Obstetrical Unit is new, and all female. They are also managing cases far beyond what their unit was set up to handle. Although the unit is a Basic Obstetrical Unit, they are providing everything except anaesthesia and caesarian section. This has come about because the local hospital refuses many of their referrals, giving as a reason that they lack the necessary equipment or personnel. Having no place to refer your difficult deliveries is guaranteed to produce dreadful outcomes. So Maggie and I agonize about how to go about an audit in these circumstances that will help them to continue to improve the services they are able to provide.
We decide not to label it as an audit, calling it instead story telling. A minor detail perhaps but it helps to contextualize it for all of us. Farida, the head of the Obstetrical Unit, agrees to set time aside for us and collects the charts and records. She has become a personal friend, which makes it both easier and more difficult. We explain again what we hope to achieve and reach agreement to focus on the stories of the referrals in the past two years.
About half way through the review, she comments, “We should do this more often, I don’t have anyone to talk to about my cases.”
I take that as a signal that it is useful for her and appreciated and my spirits lift perceptibly.
We collect the information in a systematic way, flipping through the register, the notes, the day book and drawing extensively on the Farida’s recall. She remembers each and every difficult case in detail. Her interest in her patients has, in many cases, prompted her to phone them or them to call her afterwards so we also are able to learn about many of the outcomes, which is remarkable as referral letters are almost unknown. At one point in her description of efforts to get care for delivery of conjoined twins who have presented as double footling breeches, my eyes fill up with tears.
A couple of days after our meeting with them, the lady doctors advise us they have started collecting information about each referral, which they call the stories, at the time of the referral. Farida assists us to prepare a new report form which will better capture common complications. Something that we worried would cause more problems than it would solve, turns out to be successful on many more levels than we had anticipated. It is another example of the juxtaposition of the seemingly simple and the incredibly complex. Or is it the melding of the exotic and the mundane?
I am enjoying these challenges. It feels like I am working at the fullest extension of my capabilities. At times, encouraged by what I see around me, I may even be functioning beyond my capabilities. Certainly I feel stretched. I hope, like the camel, I will be able to trod the path ahead with a surefootedness that will see me through this interesting section of the Silk Route.
Photos: camels peregrinate; ANC clinic; waiting to be seen; baby clothes; sterilizer; & fathers wait for birth.
In 2002, before I was to visit this special spot high up in the mountains outside Peshawar, a pair of bombs were dropped within Peshawar city limits by US helicopters. This served to heighten security within the whole region, so the trip was cancelled. Pakistan received an official apology a couple of days later which labeled the bombs ‘an unfortunate mistake’. It proved too late to reschedule our mountain visit.
Collateral damage, we said, a result of being too close to the Afghan border. A large exposed crater remained not far from the hotel where I was staying, providing a whole new personal perspective to the concept of “international mistakes” and “friendly fire”. The mountain site we were meant to visit was unknown to me at that time, the name Takht-i-Bhai (which sounds like Tak By) didn’t ring any bells and there was no travel guide to consult, so I wasn’t really aware of what I was missing. It is also probably true that the proximity of the bombings was distracting and I was glad enough to stay ‘close to home’, despite the obvious reminder of how dangerous “close to home” could be. The day before we leave for the mountain site this time, Maggie and I are taken to the Peshawar Museum by some friends who are unaware that we are off to visit the actual site the next day. At that point, neither of us knew we would be visiting an archaeological site or one of such significance. The tour round the museum turned out to be sheer serendipity and provides a wonderful preparation for our site visit.
The stone statues are dusty and the lighting is poor but just viewing the bits and pieces recovered from Takht-i-Bhai, I am suffused with a powerful sense of their beauty. What is even more amazing is the change in the art within the couple of hundred years on display here. Early Buddhist art portrayed the Enlightened One with symbols alone. Although conversion and holy wars were not part of Buddhism, the message and the art still managed to spread across most of Asia between the 5th and 1st century BC. It was carried along the silk routes to India and Pakistan and across monsoon-blown sea lanes to places such as Java. King Asoka, seems to have played a central role in the development of Gandhara art about the third century BC when he not only welded India into an empire but became a Buddhist convert himself. Asoka not only helped to spread Buddhism but appears to have encouraged a two-way interaction with the flourishing Greco-Roman influences around the Mediterranean.
I don’t recall having heard much about this interplay between Asian and Greco-Roman influences and find it fascinating to contemplate. It has the same fascination for me as learning about the early contact of Ethiopians with Christians and Jews. When you look at maps of both these areas, and know something of the travel routes of the day, it rings true. It also explains a great deal about how cross cultural influences happened.
The difference between the early and later Gandhara sculptures on display is striking. The raised relief of carved animals and people dance across the stone surfaces exuberantly in the later art. I would not have attributed this to its contact with the flowing forms of Greco-Roman sculpture but it is clear a major leap forward has occurred and it looks as if Buddhist art benefited most from this exchange. It sets me to thinking why this would be so and if we might be experiencing something similar in popular culture today. Much of the historical evidence of Buddhist life in the region, the great art and architecture from that period are gone. What remained intact after Alexander’s destruction were the magnificent stone Buddhas in Bamiyan. The sculptures of Bamiyan survived the destruction visited on other such sites because they were so isolated, so difficult to access and so little known. For many of us, the first we heard of the Afghanistan Buddhist treasures was in the form of worldwide outrage at the destruction visited on them by militants. Loss of these sites has made the ruins at Takht-i-Bhai even more precious. The Takht-i-Bhai site has some protection as it been designated a UNESCO World Heritage site based on its historical, religious and archeological importance. The Buddhist sanctuary, monastery and school is spread over a number of mountain sites in a area of almost 40 hectares.
On the site are the remains of a main stupa and quadrangle, a number of votive stupas, monastic court yard, lofty chapels, dining hall, meditation cells, covered passages and many other secular buildings. Most of the sculptures that remained have been removed to the Peshawar Museum. Stone walls have been created with lime and mud mortar in what is known as diaper style masonry. Original stucco and ochre-painted walls can still be found.
Maggie and I are escorted to the site by two staff members from the NGO we are visiting. They are touched by our appreciation of the site. In this ancient land it is just one more evidence of antiquity for them. We climb several of the outposts, scramble over the rocks and take pictures. The site reminds me somewhat of photos I have seen of Tibetan monasteries, high up in the clouds, spread over several different hill tops. It seems monks want the solitude and value a great view. The site has been built near and named after two wells, we are told by the Pakistani guide. We pass several young Asian women with clipboards taking notes and measurements. Our guide tells us they from a Japanese university and working on their masters. There is a guest book we are asked to sign. We flip through the back pages and note many visitors from Hong Kong and Japan. Their notes reflect the same appreciation and wonder that we have experienced. As we leave we buy a small illustrated hardcover book about the site from the Guide, glad to have some additional information.
Considering the buildings were constructed more than 800 years ago and have suffered serious attempts at destruction, the site remains remarkably alive--a touching monument to our shared and varied past.
Photos: Arial view, Peshawar Museum, Doorniche, monastary, Sole remaining Buddha, grinding stones, small pieces,
Elsewhere, World Aids Day is celebrated on Dec 7th, but in Frontier Primary Health Care (FPHC) units in North West Frontier Province of Pakistan, a whole week is devoted to spreading the word and activities are legion. Wall chalking, that will last for at least a year, is put up on walls in a number of sites, banners are strung at the entrance of each health unit, quiz competitions are held and a cricket match between men at two of the camps highlights the week long festivities. Information meetings are held for both men and women in the communities and a two special seminars have been organized for religious leaders. Staff sport homemade badges with this years WHO slogan, Keep the Promise. The youth quiz competition is won by a group of pre-teen girls attending the literacy class in the Kagan refugee camp. They pose proudly with their gold cup.
While Pakistan presently has relatively low rates of reported HIV and AIDS cases with an estimated prevalence of 0.07% in 2001, the rapidly escalating rates in neighbouring India has those concerned on edge. The risk factors in Pakistan are many. They include low condom use rates, low education and literacy especially among women, patterns of labour migration both within and outside the country that result in men living away from their families, low status of women and increasing intravenous drug abuse and commercial sex work.
A number of known risk factors are of special concern to health workers. An absence of universal blood screening results in contaminated blood and blood products that is estimated to be responsible for approximately 17.6% of current known HIV infections. Lack of appropriate infection control and waste disposal is widespread. Poor disinfection practices and lack of protective clothing such as gloves puts clients and health workers at added risk. The high number of medications given by injections by government health workers as well as traditional healers compounds the problem.
To slow the HIV epidemic, health workers and community members need to become more informed. Some of the most influential people in the community are the religious leaders. Every Friday, the entire male community gathers for noon prayers at the many mosques. The potential the religious leaders provide for wide and rapid distribution of health information is enormous. The seminars for religious leaders sponsored by FPHC are attended by 90 religious leaders from the mosques in the refugee camps and surrounding villages. The seminars have been organized for a full day. The event is hosted on the porch of the main office building in Mardan which has been screened off with stripped canvas siding. Banners proudly welcome the visitors.
The staff of FPHC are all proud multipurpose workers. They demonstrate their skills by organizing the seminars themselves. The medical storeman sweeps up the leaves in the compound. The financial officer prepares the mammoth cauldrons of meat for the noon meal. A chowkidar cooks up the biriyani in the enormous clay pot in the back yard while drivers arrange tea cups and biscuits for the morning break.
I have been joined for the final two weeks of my stay by Maggie, a colleague and friend who represents the International Health Committee of the Society of Rural Physicians of Canada. Besides the two of us, there are two other females, a pair of Master Trainers, working out of the main office. As the only females, we have been asked to keep out of sight at the back of the building. The Western toilet we normally use at the front of the building is off limits today so an Asian toilet has been marked with a Ladies sign for us.
When we come and go on our visits to the field, we are spirited by drivers through the side door. As the day wears on, it is clear that not all of the clerics read English. Maggie passes by and notices that our designated toilet has become unisex. We don't mind but we think they might not be pleased, so we make other arrangements. Yet this enforced separation is more ritual than absolute for a few of the religious leaders greet us in passing and the male staff continue to mingle easily with us.
It is however the first time Maggie and I have experienced personally the exclusion of purdah and as mild as it is, it has an impact on us. I realize I have been regarding much of the separateness of women here as somewhat self-imposed, something they choose to do, such as covering their heads, excluding men from the obstetrical wards, wearing a chador and covering their lower face in public. Most of the time as western women, Maggie and I are treated with the courtesy and protection afforded to women but also given the status of "honorary" males. This organized separation feels different and puts another perspective on the issue.
The seminars are facilitated by a local physician who is a well-known Koranic scholar. The discussion we are told has been spirited. The religious leaders are pleased to have been included in this workshop. Many of them feel they will have opportunities to educate the faithful both during Friday talks and during individual counseling sessions.
Later, a number of the questions raised by the ulema (religious leaders) are discussed with Maggie and me. They reveal an appreciation for the complexity of HIV/AIDS and a lively curiosity. A couple of queries, we have to admit we can’t answer, including how we can be sure mosquitoes will not transmit HIV when they have developed a very sophisticated means of transmitting malaria. Following the seminars, a short article is prepared by the director for the prestigious English language newspaper, The International Times. Maggie is asked to assist in editing it. As a skilled composer of op-ed pieces and news releases, she knows what is needed to get articles published. She adroitly shortens it and inserts a couple of quotes summarizing the highlights. Staff are delighted the next day when it appears in full under the byline of Our Correspondent. We tease them that they will have to submit regular articles now that they have been identified as a correspondent. It makes a fitting closure to World Aids Week in Pakistan. Photos: OfficeBanner; QuizWinners; MeatPrep; CookingRice; HC banner
A community medicine physician, I have worked for more than 30 years in Uganda, Kenya, Ethiopia, Malaysia, Laos and Pakistan. Currently I divide my time between Mbarara University of Science and Technology in Uganda and Frontier Primary Health Care, an NGO in KhyberPustoonKhwa region of Pakistan.
 Camels bearing their precious cargo, weaving in and out of traffic on the dusty highways, their colorful tassels swinging, capture for me the contradictions of our Pakistani health project. The exotic melds with the mundane. The amazingly simple rests cheek-by-jowl with the incredibly complex. And perception is in a constant dance with reality.
Camels bearing their precious cargo, weaving in and out of traffic on the dusty highways, their colorful tassels swinging, capture for me the contradictions of our Pakistani health project. The exotic melds with the mundane. The amazingly simple rests cheek-by-jowl with the incredibly complex. And perception is in a constant dance with reality.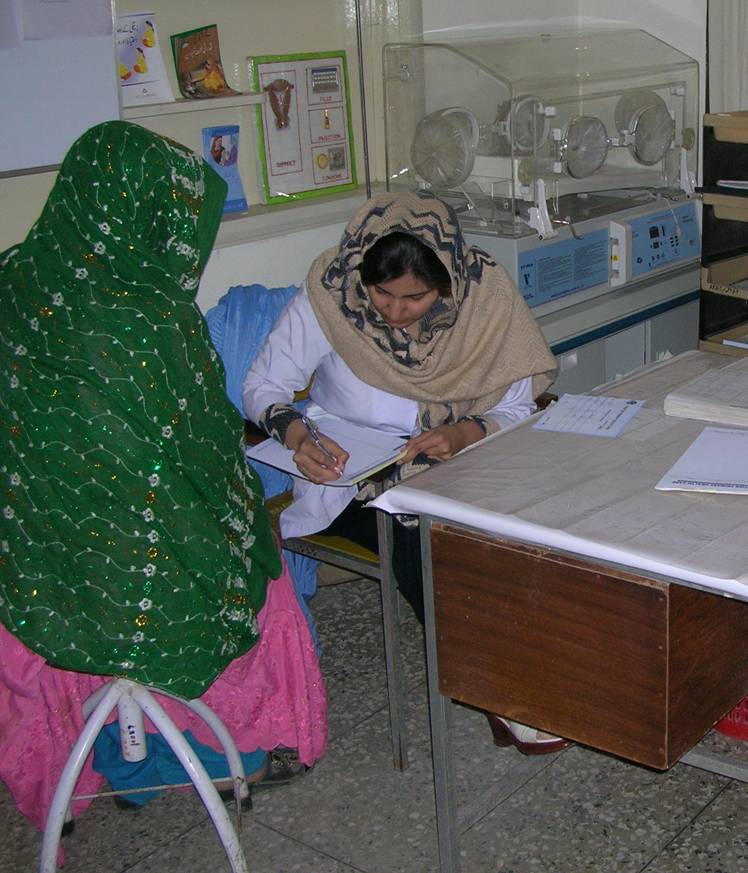

















{kind=link}
{kind=link}