Peregrinations with Camels
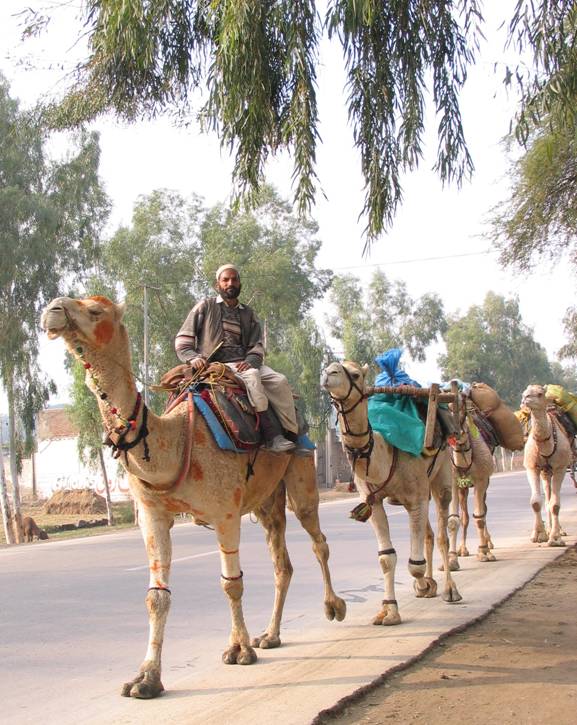 Camels bearing their precious cargo, weaving in and out of traffic on the dusty highways, their colorful tassels swinging, capture for me the contradictions of our Pakistani health project. The exotic melds with the mundane. The amazingly simple rests cheek-by-jowl with the incredibly complex. And perception is in a constant dance with reality.
Camels bearing their precious cargo, weaving in and out of traffic on the dusty highways, their colorful tassels swinging, capture for me the contradictions of our Pakistani health project. The exotic melds with the mundane. The amazingly simple rests cheek-by-jowl with the incredibly complex. And perception is in a constant dance with reality.Our project has two main goals. The first, which has a well-worked out and detailed work plan, looked initially to be the simplest. It is to strengthen the management of STD in 30 health units North Western Frontier Province of Pakistan. Because the early results from our initial baseline survey have revealed that blood products are not screened, sterilization is inadequate, placentas are handled in ways that put health workers at risk and not all health units are staffed, this seemingly simple goal may prove to be much more complicated than first envisioned.
The second goal is to build an ongoing, productive and flourishing partnership between the Canadian partner, the Society of Rural Physicians of Canada and the Pakistani partner, Frontier Primary Health Care. The second goal is somewhat more difficult to pin down and hard to measure, but may in the end prove to be the simpler. Reality and perception are in a constant, interchangeable dance around elusive truth.
Frontier Primary Health Care (FPHC) is a Pakistani Non-Government Organization (NGO) providing health care to 180,000 people in 3 different districts. They have 120 staff, 5 health centers, 3 literacy centers for young girls, a basic obstetrical unit and a Community Development Project. Frontier started in the health business with 3 Afghan refugee camps in 1981. Their success was such that they were invited to extend their services to surrounding Pakistani communities. Success in such situations is measured in part by how well health interventions manage to lower things such as maternal mortality and to improve health and treat illness in children under the age of five.
We are lucky to have such an experienced and able partner. They could do the project without Canadian input. They are used to working in a system where rigorous purdah is practiced. They utilize community and religious leaders effectively to improve health in their communities. With a committed army of both male and female volunteers, they are able to reach almost everyone in the community regularly. One of the value-added pieces that Canadian physicians can provide, they tell us, is assistance in writing funding proposals and preparing reports that would make their work better known.
For their work in refugee camps, FPHC has been funded mainly by United Nations High Commission for Refugees (UNHCR). Among the Pakistani population surrounding the camps, the medical services provided are made sustainable through modest user fees, or what is called in development parlance, “cost recovery”. Many of the Afghan refugees have been in Pakistan for more than 25 years. The younger generation of refugees has been born in Pakistan. And UNHCR is experiencing "donor fatigue", so FPHC needs to find other donors and to ensure that the services provided are sustainable and can be afforded by the population. This is both simple and complex.

It is a specific, measurable objective and therefore straight forward. Difficult, in that navigating the vicissitudes of international funders and locating appropriate donors occupies the time and energy of whole legions of people in aid agencies. If we manage to accomplish this one thing, however, we will have made our partnership worthwhile. So we already working on our next project and are on the outlook for potential donors.
Pakistan is under tight security currently so outsiders are not allowed into the refugee camps. Because Frontier PHC operates health units which are often located in the middle of the camps, staff are allowed to move to and from the health unit but not to stop in the camp enroute. During my recent visit, I was attempting to take pictures of children working in the sugar cane field and asked if we could stop on the road.
“No,” I was told sternly by staff, “We cannot stop in the camps.”
Moments later right in front of us, a donkey who was drastically overloaded, collapsed on the road, feet splayed out in front of him and would not budge. In the kafuffle that ensured, a group of laughing Afghani boys hauled on the donkey, trying to tug him upright. They placed the donkey’s legs under him, but as soon as they removed their hands, he collapsed again in a heap. Motorbikes and lorries loaded with sugar cane backed up behind us on the narrow dirt lane, beeping their horns. The donkey however was going nowhere.
Our staff laugh and tell me me that now I can take an even better picture. This is one of the contradictions of our project. Prohibitions exist and are strictly enforced but then along comes a commonplace, uncontrollable event and the situation is dramatically changed in the blink of an eye.

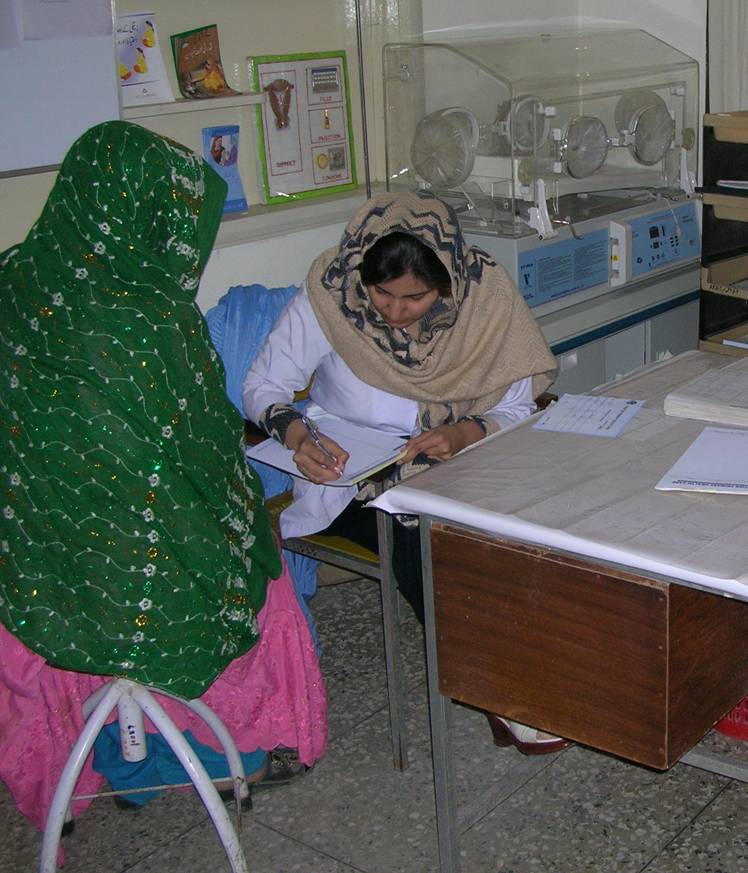
One of the things Maggie, a physician colleague, and I were asked to do during our visit was a review of obstetrical cases. A review of cases is called a medical audit. When something goes badly wrong in medical care, the result is often that someone dies or gets a complication. So audits, while necessary, can be difficult and discouraging undertakings for physicians. The staff of the Obstetrical Unit is new, and all female. They are also managing cases far beyond what their unit was set up to handle. Although the unit is a Basic Obstetrical Unit, they are providing everything except anaesthesia and caesarian section. This has come about because the local hospital refuses many of their referrals, giving as a reason that they lack the necessary equipment or personnel. Having no place to refer your difficult deliveries is guaranteed to produce dreadful outcomes. So Maggie and I agonize about how to go about an audit in these circumstances that will help them to continue to improve the services they are able to provide.
We decide not to label it as an audit, calling it instead story telling. A minor detail perhaps but it helps to contextualize it for all of us. Farida, the head of the Obstetrical Unit, agrees to set time aside for us and collects the charts and records. She has become a personal friend, which makes it both easier and more difficult. We explain again what we hope to achieve and reach agreement to focus on the stories of the referrals in the past two years.
About half way through the review, she comments, “We should do this more often, I don’t have anyone to talk to about my cases.”
I take that as a signal that it is useful for her and appreciated and my spirits lift perceptibly.
We collect the information in a systematic way, flipping through the register, the notes, the day book and drawing extensively on the Farida’s recall. She remembers each and every difficult case in detail. Her interest in her patients has, in many cases, prompted her to phone them or them to call her afterwards so we also are able to learn about many of the outcomes, which is remarkable as referral letters are almost unknown. At one point in her description of efforts to get care for delivery of conjoined twins who have presented as double footling breeches, my eyes fill up with tears.
A couple of days after our meeting with them, the lady doctors advise us they have started collecting information about each referral, which they call the stories, at the time of the referral. Farida assists us to prepare a new report form which will better capture common complications.

Something that we worried would cause more problems than it would solve, turns out to be successful on many more levels than we had anticipated. It is another example of the juxtaposition of the seemingly simple and the incredibly complex. Or is it the melding of the exotic and the mundane?
I am enjoying these challenges. It feels like I am working at the fullest extension of my capabilities. At times, encouraged by what I see around me, I may even be functioning beyond my capabilities. Certainly I feel stretched. I hope, like the camel, I will be able to trod the path ahead with a surefootedness that will see me through this interesting section of the Silk Route.
Photos: camels peregrinate; ANC clinic; waiting to be seen; baby clothes; sterilizer; & fathers wait for birth.
Labels: Pakistan
posted by Kay Wotton at 11:54 AM
![]()
![]()


3 Comments:
That is a fabulous title and an engrossing account of the "exotic and the mundane".
Regards - Shinga
Fascinating post!!! I would give a million dollars to turn a phrase like you do! : ) Great writing.
Thanks Shinga and Kim for your kind comments. When I was cut off from the blogsphere I found that I not only missed posting and wrote less but that I missed the drop by visitors and comments. We are a community of sorts even if only partly known to each other.
Post a Comment
<< Home